FIGO News 22 April 2021
We think [increased access to medical abortion] is a revolution, and women have this in their hand - it has a potential to make so many abortions in our continent safe.
Jedidah Maina
Mama network coordinator, Kenya
仮訳します
私たちは、(薬による中絶へのアクセスの向上は)革命であり、女性たちはこれを手にすることができる--私たちの大陸における非常に多くの中絶を安全にする可能性を秘めている、と考えています。
ジェディダ・マイナ
ママ・ネットワーク・コーディネーター、ケニア
On 18th March 2021, FIGO – in collaboration with the Centre for Reproductive Rights and Ipas – organised a discussion on ‘Access to medical abortion and self –managed abortion. Key insights from health workers and human rights advocates: on guaranteeing human rights’ with United Nations treaty monitoring committee members and Special Procedures mandate holders.
These elected UN experts have a responsibility to interpret human rights treaties, which includes monitoring states’ compliance with their legally binding human rights obligations and recommendations from UN experts. This includes reproductive rights and access to safe abortion. The UN experts do this by conducting fact-finding missions and issuing progress reports and statements, in addition to conducting review meetings with governments to assess their progress.
The discussion was moderated by Patty Skuster, Senior Legal Advisor at Ipas, and Christina Zampas, Associate Director, Global Advocacy at the Centre for Reproductive Rights. Ms Skuster began by clarifying the definition of medical abortion as ‘a non-invasive and highly acceptable option to pregnant persons. Medical abortion can be provided using tablets of mifepristone and misoprostol in combination or misoprostol alone,’ and the term self-managed abortion as ‘when the pregnant person finds the medication and the information on how to use it and on how to assess eligibility, progress, and outcome by themselves without the intervention of a health care provider.’
Insights were then shared by guest speakers:
Sabin Shrestha, Executive Director, Forum for Women, Law and Development, Nepal
Dr Bela Ganatra, Unit Head, Preventing Unsafe Abortion, Department of Sexual and Reproductive Health, World Health Organisation
Dr Nafissa Osman, Eduardo Mondlane University, Faculty of Medicine, Department of Obstetrics/Gynecology, Mozambique and FIGO Safe Abortion Committee member
Jedidah Maina, Executive Director, Trust for Indigenous Culture and Health (TICAH), Kenya.
Key barriers to medical and self-managed abortion
The speakers highlighted the key legal barriers to medical abortion and self-managed abortion which include:
- regulation of abortion within the penal code
- abortion medicines not registered
- requirements that abortion take place in a health facility
- requirement of health care professionals in provision of abortion care.
They provided solutions on how access to medical abortion and self-managed abortion could be strengthened for women and girls.
Reaffirming safety of medical abortion tablets
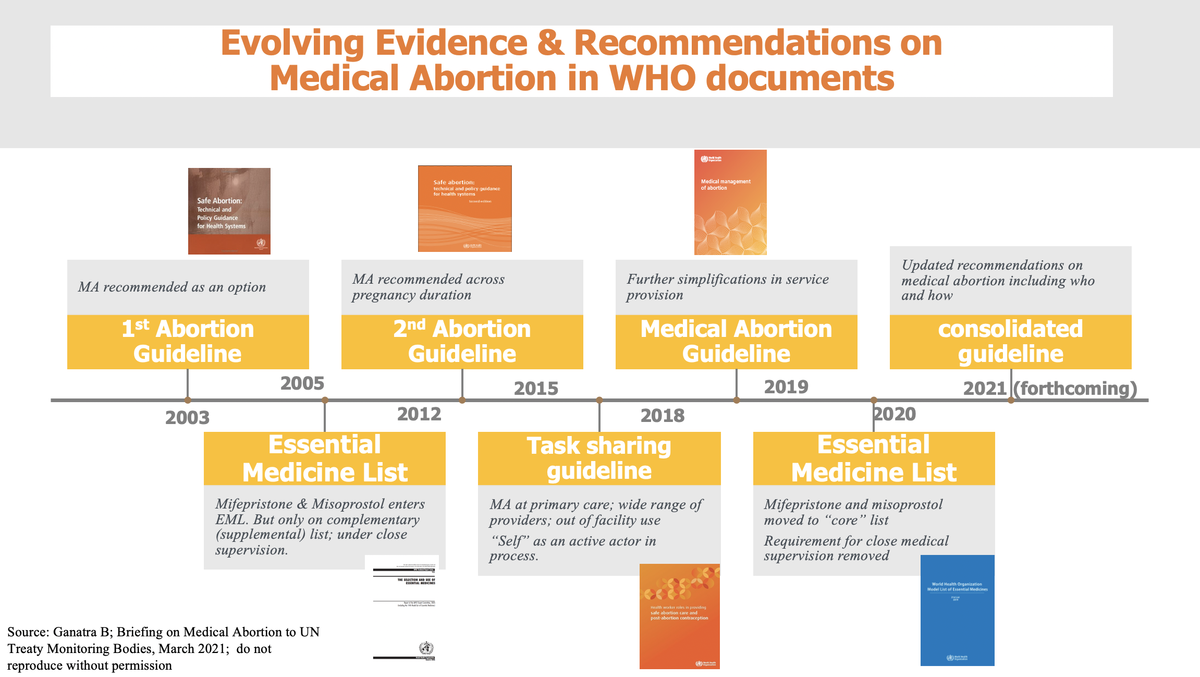
Dr Bela Ganatra reaffirmed that using medical abortion tablets mifepristone and misoprostol is an extremely safe and effective practice in both high income and low income countries. Complications using mifepristone and misoprostol are very rare and death almost negligible, and in cases where mifepristone is not available then misoprostol could be used alone:
‘There is a large body of evidence on safety and efficacy of medical abortion from all over the world - both from high and low income countries….Mifepristone and misoprostol have been moved to the “core” Essential Medicine List and the requirement for close medical supervision is removed.’
Dr Ganatra presented a visual timeline of the evolving evidence and recommendations on medical abortion from WHO.
medical abortion recommendation timeline WHO
Dr Ganatra stressed that the science on who can provide the medical abortion tablets and under what conditions medical abortion tables can be provided has been progressively evolving over the last 20 years. WHO guidelines from 2015 already identified the various roles of different health care providers, including lay workers and pharmacists and the pregnant person themselves in different aspects of abortion care. Since then, more scientific evidence has been generated on this topic and work is ongoing to update these recommendations. The new WHO abortion guidelines are likely to be available later in the year (also see current WHO abortion guidelines).
Dr Nafissa Osman provided key insights from the perspective of Africa and specifically her home country, Mozambique. She began by highlighting how 25 million unsafe abortions took place each year between 2010 and 2014, and that 45% of all abortions are unsafe. 97% of unsafe abortions take place in Africa, Asia and Latin America, and the risk of dying from an unsafe abortion is highest in Africa.
Drawing on clinical evidence, Dr Osman reaffirmed:
‘Medical abortion is a very safe treatment and in clinical trials, success rates are between 92.5% and 100% depending on gestational age, the time interval between Mifepristone and Misoprostol, the misoprostol administration route and doses.’
Yet, while medical abortion is very safe, Dr Osman highlighted that in Africa there is still much to do to make access to safe abortion a reality for women and girls. Only 3 of 55 African countries allowed abortion upon request (up to varying pregnancy durations). These are Mozambique, South Africa and Tunisia.
But even when abortion is available upon request there are often barriers to access. For example, in Mozambique, abortion must be carried out in the health units of the National Health Service, by health professionals, and requires sign-off/approval from health workers. Such protocols serve as barriers in ensuring access to abortion for women and girls, especially the more marginalised.
‘There are many barriers/challenges to accessing abortion at the health facility level. This includes the implementation of the law, policies and guidelines which is often slow, the role of service-providers’ own personal values, beliefs, and attitudes which may stigmatise women/girls requiring an abortion, and the lack of functional safe abortion services (including trained staff, supply of drugs) – includes the availability of free, accessible and acceptable safe abortion service… These barriers then adversely impact marginalised women/girls' access to safe abortion, especially those from poor and marginalised sectors who are at greater risk to high levels of violence and unsafe abortion.’
Dr Osman concluded her presentation by stating that FIGO endorsed the permanent adoption of telemedicine abortion services, which is a safe and private method to have an abortion in early pregnancy without having to visit a clinic. It helps to reduce exposure to stigma and increases access to abortion services for women and girls living in remote communities.
Sabin Shrestha, Nepal, shared that despite access to abortion being recognised as a fundamental right in Nepal’s Constitution and enacted in Nepal’s legislation, women and girls were still being imprisoned if they took medical abortion tablets from a health service provider and/or health setting not on the government's approved list. He shared the case details of a 15-year-old (minor) rape survivor who had been arrested and imprisoned for taking medical abortion tablets that had been provided by her father via a pharmacist.
Jedidah Maina, Kenya, who coordinates the Mama Network, a grass-roots activist network that works to expand medical abortion across Africa and operates in 17 sub-Saharan African countries, stated that:
‘There continues to be cultural taboos that prevent open dialogue in homes and in school and sometimes our laws and policies do not mirror the lived realities of women/girls… the law criminalises self-care/abortion management… We [Mama network] increase access to medical abortion as a safe, effective medical procedure outside a clinical setting… we think this is a revolution, and women have this in their hand – it has the potential to make so many abortions in our continent safe and that States need to adapt their laws to reflect this lived reality of people who have abortions.’
Questions that UN experts should raise with governments
The discussion concluded with specific questions that UN experts could raise with governments when assessing their progress on ensuring access to safe abortion. These included:Is medical abortion legal and available in your country? If it is legal, is it regulated in an appropriate way for the intended use and to enable self-managed abortion, or is it regulated under frameworks intended for surgical or vacuum aspiration?
Are the drugs misoprostol and mifepristone registered and included on the National list of essential medicines? If yes, is misoprostol used for abortions?
Do the regulations allow for telemedicine/health in your country? Are they read to include medical abortion services?
Does the law contain requirements that result in criminalisation of abortions that are obtained outside the formal health care setting?
Do abortion providers or individuals who seek abortion experience arrest, harassment, bribery, or criminal penalties related to abortion?
The attendees (UN experts) were also encouraged to advocate that all governments decriminalise all abortions by completely removing abortion and any regulation of abortion from criminal or penal codes. Further details on the recommendations that UN experts could advocate for are available from the meeting presentation, and you are able to watch the recording here.FIGO urges its member societies to utilise these recommendations in your advocacy with governments and stakeholders, in order to strengthen advocacy for safe abortion within your national contexts.
仮訳します。
2021年3月18日、FIGOは、リプロダクティブ・ライツ・センターおよびIpasと共同で、「薬による中絶と自己管理による中絶へのアクセス」に関する討論会を開催した。医療従事者と人権擁護者からの重要な洞察:人権の保障について」と題し、国連条約監視委員会委員と特別手続きのマンデートホルダーを交えたディスカッションを行いました。
これらの選出された国連専門家は、人権条約を解釈する責任を負っており、これには国家が法的拘束力のある人権義務や国連専門家の勧告を遵守しているかどうかを監視することも含まれる。これには、リプロダクティブ・ライツや安全な中絶へのアクセスも含まれます。国連の専門家は、事実調査団を派遣し、進捗状況報告書や声明を発表するほか、政府との検討会議を行い、進捗状況を評価することによって、これを実現しています。
ディスカッションは、Ipasのシニア・リーガル・アドバイザーであるPatty Skuster氏と、Centre for Reproductive Rightsのグローバル・アドボカシー担当アソシエイト・ディレクターであるChristina Zampas氏がモデレーターを務めました。Skusterはまず、薬による中絶の定義を「妊娠中の人にとって非侵襲的で、非常に受け入れやすい選択肢」と明確にしました。薬による中絶は、ミフェプリストンとミソプロストールの錠剤を組み合わせて、あるいはミソプロストール単独で行うことができます」そして、自己管理による中絶とは、「妊娠中の人が医療従事者の介入なしに、薬とその使用方法、資格、経過、結果の評価方法に関する情報を自分で見つける場合」であると述べました。
続いて、ゲストスピーカーによる見識の共有が行われました。
サビン・シュレスタ(ネパール、女性・法・開発フォーラム、事務局長
世界保健機関(WHO) 性と生殖に関する健康部 安全でない人工妊娠中絶の防止ユニット責任者 ベラ・ガナトラ博士
ナフィッサ・オスマン博士、エドゥアルド・モンドラーネ大学医学部産科婦人科学科、モザンビーク、FIGO安全な妊娠中絶委員会委員
ジェディダ・マイナ(ケニア、先住民文化と健康のための信託(TICAH)、エグゼクティブディレクター
薬による中絶と自己管理による中絶に対する主な障壁
講演者は、薬による中絶と自己管理による中絶に対する主な法的障害に焦点を当てました。
- 刑法における中絶の規制
- 登録されていない中絶薬
- 中絶は医療施設で行われなければならない。
- 中絶を行うには、医療従事者が必要であること。
また、女性や少女のために薬による中絶や自己管理による中絶へのアクセスをどのように強化できるかについての解決策を提供しました。
薬による中絶の錠剤の安全性の再確認
ベラ・ガナトラ博士は、薬による中絶の錠剤であるミフェプリストンとミソプロストールを使用することは、高所得国でも低所得国でも非常に安全で効果的な方法であることを再確認しました。ミフェプリストンとミソプロストールを用いた合併症は非常に稀で、死亡はほとんど無視できるほどです。
薬による中絶の安全性と有効性については、高所得国、低所得国を問わず、世界中から多くの証拠が集まっています。ミフェプリストンとミソプロストールは、「中核」必須医薬品リストに移動し、厳重な医学的管理の必要性が取り除かれました。
ガナトラ博士は、WHOによる薬による中絶に関する進化する証拠と勧告の視覚的な年表を発表しました。
薬による中絶の勧告のタイムライン WHO
ガナトラ博士は、誰が薬による中絶錠を提供できるか、どのような条件の下で薬による中絶錠を提供できるかに関する科学は、この20年間で徐々に進化してきたと強調しました。2015年のWHOガイドラインでは、すでに中絶ケアのさまざまな側面において、一般人や薬剤師を含むさまざまな医療従事者、そして妊娠者本人の役割が確認されています。それ以来、このテーマについてより多くの科学的な証拠が生み出され、これらの勧告を更新する作業が進行中です。新しいWHO中絶ガイドラインは、今年後半に利用可能になるようです(現行のWHO中絶ガイドラインもご参照ください)。ナフィッサ・オスマン博士は、アフリカ、特に彼女の母国であるモザンビークの観点から、重要な洞察を述べました。彼女はまず、2010年から2014年の間に毎年2500万件の危険な中絶が行われ、全中絶の45%が危険な中絶であることを強調しました。危険な中絶の97%はアフリカ、アジア、ラテンアメリカで行われており、危険な中絶で死亡するリスクはアフリカで最も高いのです。
臨床的な証拠をもとに、オスマン医師は再確認しました。
薬による中絶は非常に安全な治療法であり、臨床試験では、妊娠年齢、ミフェプリストンとミソプロストールの投与間隔、ミソプロストールの投与経路や投与量によって、成功率は92.5%から100%です」。
しかし、薬による中絶は非常に安全ですが、オスマン博士は、アフリカでは女性や少女が安全な中絶を利用できるようにするためにまだやるべきことがたくさんあることを強調しました。アフリカの55カ国のうち3カ国だけが、要求に応じて中絶を許可していました(妊娠期間の長短はありますが)。モザンビーク、南アフリカ、チュニジアである。
しかし、希望により中絶が可能な場合でも、アクセスに障壁があることが多い。例えば、モザンビークでは、中絶は国民保健サービスの保健ユニットで、医療専門家によって行われなければならず、医療従事者のサインオフや承認が必要です。このようなプロトコルは、女性や少女、特に社会から疎外されている人々の中絶へのアクセスを確保する上で障壁となる。
「医療施設レベルでの中絶へのアクセスには多くの障壁や課題があります。これには、法律、政策、ガイドラインの実施にしばしば時間がかかること、サービス提供者自身の個人的な価値観、信念、中絶を必要とする女性/少女にスティグマを与えるかもしれない態度の役割、機能的な安全中絶サービスの欠如(訓練を受けたスタッフ、薬物の供給など)-無料、アクセス、許容できる安全中絶サービスの利用を含む...があります。これらの障壁は、社会から疎外された女性/少女の安全な中絶へのアクセス、特に高いレベルの暴力や危険な中絶のリスクがより高い貧困層や社会から疎外された層の女性/少女に悪影響を及ぼします。 '
遠隔医療は、妊娠初期にクリニックを訪れることなく中絶を行うための安全で個人的な方法です。遠隔医療は、スティグマにさらされることを減らし、遠隔地に住む女性や少女が中絶サービスを受けられるようにします。
ネパールのサビン・シュレスタさんは、中絶へのアクセスがネパール憲法で基本的権利として認められ、ネパールの法律で制定されているにもかかわらず、女性や少女が政府の承認リストにない医療サービス提供者や医療施設から薬用中絶錠を服用すると投獄されることがあると話しました。彼は、15歳のレイプ被害者(未成年)が、父親から薬剤師を通じて提供された薬用中絶錠剤を服用したために逮捕され、投獄されたという事例の詳細を紹介しました。
アフリカ全土に薬による中絶を拡大するために活動し、サハラ以南のアフリカ17カ国で活動している草の根活動家ネットワーク「ママ・ネットワーク」をコーディネートするケニアのジェディダ・マイナ氏は、次のように述べています。
家庭や学校でのオープンな対話を妨げる文化的タブーがあり続け、私たちの法律や政策が女性/少女の生活実態を反映していないこともあります...法律はセルフケア/中絶管理を犯罪としています...私たち(ママネットワーク)は、臨床現場以外の安全で効果的な医療行為としての薬による中絶へのアクセスを増やします...」と述べています。これは革命であり、女性たちはこれを手にしています。私たちの大陸の多くの中絶を安全にする可能性を秘めています。 '
国連専門家が政府に提起すべき質問
議論の最後には、国連の専門家が、安全な中絶へのアクセスを確保するための進捗状況を評価する際に、各国政府に提示すべき具体的な質問事項が挙げられた。その内容は以下の通りです。
- あなたの国では、薬による中絶は合法で利用できますか?
- 薬による中絶が合法であり、利用可能か?
- 合法である場合、それは意図された用途と自己管理による中絶を可能にするために適切な方法で規制されているか、または外科手術や真空吸引を目的とした枠組みのもとで規制されているか?
- ミソプロストールとミフェプリストンが登録され、国の必須医薬品リストに含まれていますか?
- 登録されている場合、ミソプロストールは中絶に使用されていますか?
- あなたの国では、規制によって遠隔医療や健康が認められていますか?
- 薬による中絶のサービスを含むように読み取れますか?
- 法律には、正式な医療の場以外で行われる中絶を犯罪とするような要件が含まれているか?
- 中絶を提供する人や中絶を求める人は、中絶に関連した逮捕、嫌がらせ、贈収賄、刑事罰などを経験していますか?
また、出席者(国連専門家)は、すべての政府が、中絶と中絶に関するあらゆる規制を刑法や刑罰規定から完全に取り除くことによって、すべての中絶を非犯罪化することを提唱するよう促されました。国連専門家が提唱できる提言の詳細は、会議のプレゼンテーションから入手可能であり、その録画はここで見ることができます。
FIGOは、加盟団体に対し、自国の状況において安全な中絶のためのアドボカシーを強化するために、政府や関係者とのアドボカシーにおいてこれらの勧告を利用するよう促します。